
Sample Informed Consent Related Documents
For educational purposes only
Key Information Page Examples for Simulated Studies
Comparative Effectiveness Research
KEY INFORMATION FOR A COMPARATIVE STUDY OF TWO DRUGS
We want to compare two medicines used to treat Chronic Obstructive Lung Disease (COPD). COPD makes it hard to breathe because of lung damage. We are inviting you to take part in a research study because your lung doctor diagnosed you with COPD.
WHAT IS THE PURPOSE, PROCEDURES, AND DURATION OF THIS STUDY?
We do not know if Drug A or Drug B is better at improving Health Related Quality of Life (HRQoL) in COPD patients. We hope to learn which medicine will help you breathe better.
If you agree to participate:

WHAT ARE REASONS YOU MIGHT CHOOSE NOT TO VOLUNTEER FOR THIS STUDY?
You may not benefit personally. You will not be able to choose which group you will be in. You may experience side effects from the drug you are given.
WHAT ARE REASONS YOU MIGHT CHOOSE TO VOLUNTEER FOR THIS STUDY?
The Food and Drug Administration (FDA) approved both medicines used in this study to treat COPD. The study provides the medicine and research visits to you at no cost.
DO YOU HAVE TO TAKE PART IN THE STUDY?
You do not have to be in the study to receive medicine for your COPD. Drug A and Drug B are available outside of the study. You can withdraw from the study at any time.
WHAT IF YOU HAVE QUESTIONS, PROBLEMS, SUGGESTIONS, OR CONCERNS?
If you have questions about this study, you can contact: (email and phone number).
If you have any questions or concerns about your rights as a research volunteer, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI), Monday – Friday, 8 am - 5 pm EST, at 859-257-9428 or toll-free at 1-866-400-9428.
Continue on to the detailed consent

Placebo-Controlled Clinical Trial
Consent and Authorization to Participate in a Research Study
KEY INFORMATION FOR: Randomized, Placebo-Controlled Trial to assess the safety and effectiveness of Investigational E-FLEX in the treatment of Arthritis
We are asking you to choose whether to take part in a clinical research study that will test the benefits and safety of E-FLEX stiff in patients with Arthritis. This page is to give you key information to help you decide whether to participate. We have included detailed information after this page. Ask the research team questions. If you have questions later, the contact information for the research investigator in charge of the study is below.
WHAT IS THE PURPOSE, PROCEDURES, AND DURATION OF THIS STUDY?
The purpose of this study is to compare the effects, good and/or bad, of E-FLEX with a placebo (an inactive pill). The Food and Drug Administration (FDA) has approved E-FLEX to treat some conditions. FDA has not approved E-FLEX to treat arthritis.
If you are eligible for the study, we will use a computer program to place you in one of the two groups. The group the computer picks is by chance, like flipping a coin. You will have an equal chance of getting into either group. The test group will take E-FLEX. The placebo group will take an inactive pill. Neither you nor the study staff will know to which pill you get. They both look the same. Participants in both groups will have monthly research study visits for one (1) year. See Appendix A for the study visit schedule.
WHAT ARE REASONS YOU MIGHT CHOOSE TO VOLUNTEER FOR THIS STUDY?
Some doctors have noticed an improvement in arthritis in patients taking E-FLEX. While on the study, we will monitor your arthritis. If your arthritis worsens, the study doctor may take you off the study so that your personal doctor may treat you.
The study will provide the E-FLEX or placebo pill, research tests, and care at no cost to you. The detailed consent has a complete description of possible study benefits. In addition, we will teach all study participants skills and lifestyle changes that help manage arthritis.
WHAT ARE REASONS YOU MIGHT CHOOSE NOT TO VOLUNTEER FOR THIS STUDY?
You may decide that you do not want to participate in this study because there is a chance the study computer will place you in the placebo group. If you are in the placebo group, you will take a pill daily for one year that will not help your arthritis. If the study computer places you in the test group, there is no guarantee that E-FLEX will help your arthritis. Research has not been done to confirm whether it will improve arthritis.
You may have side effects while on the study. The most serious effect that has happened in one percent of people who have taken E-FLEX is shortness of breath. The researchers do not know all of the side effects that could happen. Appendix B lists the type and rate of known side effects from taking E-FLEX.
DO YOU HAVE TO TAKE PART IN THE STUDY?
If you decide to take part, it should be because you really want to volunteer. You will not lose any benefits or rights you would normally have if you choose not to volunteer. You can withdraw at any time during the study.
WHAT IF YOU HAVE QUESTIONS, SUGGESTIONS, OR CONCERNS?
The person in charge of this study is Arthur Young, MD. If you have questions or concerns regarding this study or you want to withdraw from the study, their contact information is: researcher@uky or xxx-xxx-xxxx.
If you have any questions, suggestions, or concerns about your rights as a volunteer in this research, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI) between the business hours of 8 am and 5 pm EST, Monday-Friday, at 859-257-9428 or toll-free at 1-866-400-9428.

Continue on to the detailed consent

Research Biobank
KEY INFORMATION FOR THE ACME SAMPLE BANK
We are inviting you to take part in a research sample bank. We want to learn about the role genes play in health and disease.
WHAT IS THE PURPOSE, PROCEDURES, AND DURATION OF THIS STUDY?
The purpose of the sample bank is to collect and store specimens for research in the future. We will collect a small sample of blood, urine, nails, hair, and saliva. The bank will store the samples and your personal and health information forever. Both the researchers managing the bank and other researchers at UK will do studies with your samples. Future research may include lab studies, animal research, or genetic testing.

WHAT ARE REASONS YOU MIGHT CHOOSE TO VOLUNTEER FOR THIS STUDY?
- You may like knowing you contributed to research that may help others in the future. For example, genetic sample studies explain how disease traits are passed down in families.
- The bank will take steps to keep your information confidential. We will remove information that could identify you before sharing it with researchers.
- Genetic information is unique to you. There are laws that make it illegal to discriminate against you based on your genetic information.
WHAT ARE REASONS YOU MIGHT CHOOSE NOT TO VOLUNTEER FOR THIS STUDY?
- You will not benefit personally, medically, or financially. The samples you donate no longer belong to you.
- You will not receive the results from future research tests.
- Future advances in technology could make it possible to identify you from the genetic tests. We cannot promise your identity will stay private.
DO YOU HAVE TO TAKE PART IN THE STUDY?
You should only take part in our research study if you want to. You will not lose any services, benefits, or rights you would normally have if you choose not to volunteer.
WHAT IF YOU HAVE QUESTIONS, SUGGESTIONS OR CONCERNS?
The person in charge of this research bank is (name). You can contact (name) if you have questions or concerns about the bank here: (phone/email).
If you have any questions or concerns about your rights as a volunteer in this research, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI) between the business hours of 8 am and 5 pm EST, Monday-Friday at 859-257-9428 or toll-free at 1-866-400-9428.

Clinical Outcomes
Consent and Authorization to Participate in a Research Study
KEY INFORMATION FOR ANALGESIC EFFICACY FOR INTRAVITREAL INJECTIONS
We are asking you to choose whether to volunteer for a research study about numbing the eye before eye injections. We are asking you because you are getting an eye injection and need numbing medicine first. This page is to give you key information to help you decide if you want to take part. There is detailed information after this page. Ask the research team questions. If you have questions later, you can use the bold phone number or email address at the bottom of this page to talk to the person in charge of this study.
WHAT IS THE STUDY ABOUT?
We hope this study will help us find out the best way to numb the eye before an eye injection and make our clinic practice better. We will record information about:
- the medicines we use
- how we numb your eye
- your pain level for the injection
- some personal information (like age, race, etc.)
This study will not affect which treatment you get today.
AND HOW LONG WILL IT LAST?
Your part in this study will last about 1 hour, the length of your visit today.
WHAT ARE SOME REASONS YOU MIGHT WANT TO VOLUNTEER?
You might want to volunteer for this study because it could help us learn the best way to numb the eye before eye injections.
WHAT ARE SOME REASONS YOU MIGHT NOT WANT TO VOLUNTEER?
You might not want to volunteer if:
- You don’t want us to keep and use your information
- You don’t want to answer questions during today’s visit
DO I HAVE TO TAKE PART?
No, you do not have to take part in this study. If you volunteer, it should be because you really want to. You will not lose any rights, services, or benefits if you choose not to take part in this study.
WHAT IF I HAVE QUESTIONS? CONCERNS? SUGGESTIONS?
The person in charge of the study is {enter PI name}, MD, of the University of Kentucky Department of {enter department name}. If you have questions, concerns, or suggestions about this study or you want to stop being in the study, contact him/her at name@uky.edu or 859‐XXX‐XXXX.
If you have any questions or concerns about your rights as a volunteer in this research, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI) between the business hours of 8 am and 5 pm EST, Monday-Friday, at 859-257-9428 or toll-free at 1-866-400-9428.

Healthy Volunteer Medical

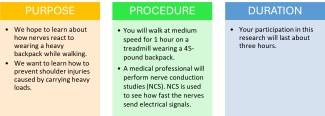
KEY INFORMATION FOR THE EFFECT OF LOAD BEARING AND
RECOVERY OF SHOULDER FUNCTION
We are inviting you to take part in a research study about the effects of heavy loads on shoulder function. Healthy individuals, aged 18 to 30, who pass a fitness screening are eligible to participate.
WHAT ARE REASONS YOU MIGHT CHOOSE TO VOLUNTEER FOR THIS STUDY?
- Some participants appreciate knowing they contributed to research that may benefit others in the future.
- You can stop at any time if you experience pain or feel bad during the study.
- Medical professionals will perform the screening and the tests. For a complete description of potential benefits, refer to the Detailed Consent that follows.
WHAT ARE REASONS YOU MIGHT CHOOSE NOT TO VOLUNTEER FOR THIS STUDY?
- You may not benefit directly from this study.
- You may feel burning muscle pain or twitching from the NCS.
- You may feel tired or sore from walking on the treadmill.
- The backpack could cause muscle strain during the 1-hour exercise.
DO YOU HAVE TO TAKE PART IN THE STUDY?
If you decide to take part in the study, it should be because you really want to volunteer. You will not lose any services, benefits or rights you would normally have if you choose not to volunteer.
WHAT IF YOU HAVE QUESTIONS, SUGGESTIONS, OR CONCERNS?
The person in charge of this study is (name) of the University of Kentucky. Contact (name) if you have questions or concerns, or you want to withdraw from the study: (name, contact information).
If you have any questions or concerns about your rights as a volunteer in this research, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI) between the business hours of 8 am and 5 pm EST, Monday-Friday, at 859-257-9428 or toll-free at 1-866-400-9428.
Continue to the Detailed Consent

Healthy Volunteer Nonmedical
RELAXATION AND ACADEMIC OUTCOMES STUDY
We are inviting you to take part in a research study about how the X relaxation method affects the grades of university students. X is a relaxation method that uses controlled breathing and sensory focus. We plan to enroll 25 healthy students who are not taking prescription or over-the- counter medication for anxiety or depression.
PURPOSE: We want to learn how students use the X relaxation method to improve grades.
PROCEDURE:

DURATION: Your participation in this research will last one semester.
REASONS YOU MIGHT CHOOSE TO VOLUNTEER FOR THIS STUDY
- You may experience more control over your life and better academic focus.
- You may like knowing you contributed to research that may benefit others.
- You will be compensated for the time you spend completing the surveys.
REASONS YOU MIGHT CHOOSE NOT TO VOLUNTEER FOR THIS STUDY
- You do not get to choose your study group.
- Participation in the test group will require more time to complete weekly logs.
- You may not want to stop taking dietary supplements during the study.
DO YOU HAVE TO TAKE PART IN THE STUDY?
You do not have to be in the study. You will not lose normal services, benefits, or rights if you choose not to be in the study.
WHAT IF YOU HAVE QUESTIONS, SUGGESTIONS, OR CONCERNS?
The person in charge of this study is (name) of the University of Kentucky. You can contact (name) if you have questions or concerns here: (name, information).
If you have any questions or concerns about your rights as a volunteer in this research, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI) between the business hours of 8 am and 5 pm EST, Monday-Friday, at 859-257-9428 or toll-free at 1-866-400-9428.

Nonmedical testing and survey
HORROR GAMES AND PERCEPTIONS OF REALITY
WE ARE INVITING YOU TO TAKE PART IN A RESEARCH STUDY ON THE EFFECTS OF PLAYING HORROR VIDEO GAMES. YOU MAY TAKE PART IN THE STUDY IF YOU ARE HEALTHY AND OVER 18 YEARS OLD. AND YOU PLAY HORROR VIDEO GAMES AT LEAST TWICE A WEEK.
PURPOSE, PROCEDURE & DURATION
We want to know how game players view the world around them after playing a lot of horror video games. We will ask you to take part in a short horror gameplay session. Then, you will complete a survey. The survey will take about 1 hour.
YOU MIGHT WANT TO BE IN THE STUDY
- You might help us learn how video games affect behavior and attitude.
- You will experience no more risk of harm than you would in everyday life.
YOU MIGHT NOT WANT TO BE IN THE STUDY
- You might not benefit directly from this research study.
- Flashing lights and moving patterns may bother you.
- You may feel upset after playing horror video games.
DO YOU HAVE TO BE IN THE STUDY?
You do not have to be in the study. You will not lose normal services, benefits, or rights if you choose not to be in the study.
WHAT IF YOU HAVE QUESTIONS?
The person in charge of this study is (name) of the University of Kentucky. You can contact (name) if you have questions or concerns here: (name, information).

Other Informed Consent-related Documents
Parent Permission Sample
Key Information Page:
Consent to Participate in a Research Study
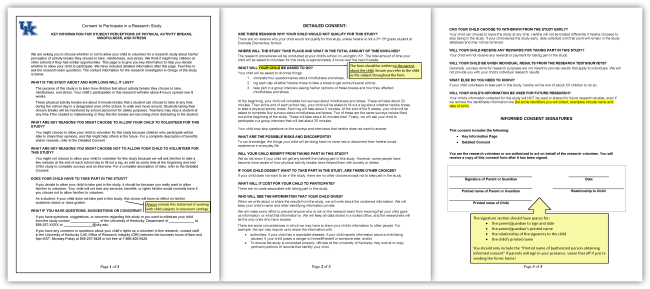
KEY INFORMATION FOR STUDENT PERCEPTIONS OF PHYSICAL ACTIVITY BREAKS, MINDFULNESS, AND STRESS
We are asking you to choose whether or not to allow your child to volunteer for a research study about their perception of activity breaks they choose to take, mindfulness, and stress. We think it might help children at other schools if they had similar opportunities. This page is to give you key information to help you decide whether to allow your child to participate. We have included detailed information after this page. Feel free to ask the research team questions. The contact information for the research investigator in charge of the study is below.
WHAT IS THE STUDY ABOUT AND HOW LONG WILL IT LAST?
The purpose of this study is to learn how children feel about activity breaks they choose to take, mindfulness, and stress. Your child's participation in this research will take about 4 hours spread over 6 weeks.
These physical activity breaks are about 5-minute breaks that a student can choose to take at any time during the school day in a designated area of the school, to walk and move around. Students taking their chosen breaks will be monitored by school personnel for safety purposes. Teachers may stop a student at any time if the student is misbehaving or they feel the breaks are becoming more distracting to the student.
WHAT ARE KEY REASONS YOU MIGHT CHOOSE TO ALLOW YOUR CHILD TO VOLUNTEER FOR THIS STUDY?
You might choose to allow your child to volunteer for this study because children who participate will be able to share their opinions, and this might help others in the future. For a complete description of benefits and/or rewards, refer to the Detailed Consent.
WHAT ARE KEY REASONS YOU MIGHT CHOOSE NOT TO ALLOW YOUR CHILD TO VOLUNTEER FOR THIS STUDY?
You might not choose to allow your child to volunteer for this study because we will ask them to take a few minutes at the end of each school day to fill out a log, as well as some time at the beginning and end of the study to complete surveys and an interview. For a complete description of risks, refer to the Detailed Consent.
DOES YOUR CHILD HAVE TO TAKE PART IN THE STUDY?
If you decide to allow your child to take part in the study, it should be because you really want to allow them to volunteer. Your child will not lose any services, benefits, or rights they would normally have if you choose not to allow them to volunteer.

As a student, if your child does not take part in this study, this choice will not affect their academic status or class grades.
WHAT IF YOU HAVE QUESTIONS, SUGGESTIONS, OR CONCERNS?
If you have questions, suggestions, or concerns regarding this study or you want to withdraw your child from the study, contact (name) of the University of Kentucky, Department of (department name) at 859-257-XXXX or XXXX@uky.edu.
If you have any questions or concerns about your rights as a volunteer in this research, contact staff in the University of Kentucky (UK) Office of Research Integrity (ORI) between the business hours of 8 am and 5 pm EST, Monday-Friday, at 859-257-9428 or toll-free at 1-866-400-9428.
Detailed Consent:
DETAILED CONSENT:
ARE THERE REASONS WHY YOUR CHILD WOULD NOT QUALIFY FOR THIS STUDY?
There are no reasons why your child would not qualify for this study unless they are not a 3rd -5th grade student at Example Elementary School.
WHERE WILL THE STUDY TAKE PLACE, AND WHAT IS THE TOTAL AMOUNT OF TIME INVOLVED?
The research procedures will be conducted at your child’s school in Lexington, KY. The total amount of time your child will be asked to volunteer for this study is approximately 4 hours over the next 6 weeks.
WHAT WILL YOUR CHILD BE ASKED TO DO?

Your child will be asked to do three things:
- Complete four questionnaires about mindfulness and stress,
- Log each day whether they chose to take a break to get some physical activity,
- Take part in a group interview, asking their opinions on these breaks and how they affected mindfulness and stress.
At the beginning, your child will complete two surveys about mindfulness and stress. These will take about 20 minutes. Then, at the end of each school day, your child will be asked to fill out a log about whether they chose to take a physical activity break. Each log will take about 5 minutes. At the end of the 6 weeks, your child will be asked to complete four surveys about mindfulness and stress. Two of these are the same surveys they filled out at the beginning of the study. These will take about 40 minutes total. Finally, we will ask your child to participate in a group interview that will last about 30 minutes.
Your child may skip questions on the surveys and interviews that they do not want to answer.
WHAT ARE THE POSSIBLE RISKS AND DISCOMFORTS?
To our knowledge, the things your child will be doing have no more risk or discomfort than they would experience in everyday life.
WILL YOUR CHILD BENEFIT FROM TAKING PART IN THIS STUDY?
We do not know if your child will get any benefit from taking part in this study. However, some people have become more aware of how physical activity breaks have helped them with anxiety or stress.
IF YOUR CHILD DOESN’T WANT TO TAKE PART IN THE STUDY, ARE THERE OTHER CHOICES?
If your child does not want to be in the study, there are no other choices except not to take part in the study.
WHAT WILL IT COST FOR YOUR CHILD TO PARTICIPATE?
There are no costs associated with taking part in this study.
WHO WILL SEE THE INFORMATION THAT YOUR CHILD GIVES?
When we write about or share the results from the study, we will write about the combined information. We will keep your child’s name and other identifying information private.
We will make every effort to prevent anyone who is not on the research team from knowing that your child gave us information or what that information is. We will keep all data stored in a locked office, and the researchers will be the only ones who have access.
There are some circumstances in which we may have to show your child’s information to other people. For example, the law may require us to share the information with:
- Authorities, if your child has a reportable disease, if your child reports information about a child being abused, if your child poses a danger to themself or someone else; and/or
- To ensure the study is conducted properly, officials at the University of Kentucky may look at or copy pertinent portions of records that identify your child.
CAN YOUR CHILD CHOOSE TO WITHDRAW FROM THE STUDY EARLY?
Your child can choose to leave the study at any time. They will not be treated differently if they choose to stop being in the study. If your child leaves the study early, data collected until that point will remain in the study database and may not be removed.
WILL YOUR CHILD RECEIVE ANY REWARDS FOR TAKING PART IN THIS STUDY?
Your child will not receive any rewards or payment for taking part in the study.
WILL YOUR CHILD BE GIVEN INDIVIDUAL RESULTS FROM THE RESEARCH TESTS/SURVEYS?
Generally, surveys done for research purposes are not meant to provide results that apply to individuals. We will not provide you with your child’s individual research results.
WHAT ELSE DO YOU NEED TO KNOW?
If your child volunteers to take part in this study, they will be one of about XX children to do so.
WILL YOUR CHILD’S INFORMATION BE USED FOR FUTURE RESEARCH?
Your child’s information collected for this study will NOT be used or shared for future research studies, even if we remove the identifiable information like [list some identifiers you will collect; examples include name and date of birth].
INFORMED CONSENT SIGNATURES
This consent includes the following:
- Key Information Page
- Detailed Consent
You are the research volunteer or are authorized to act on behalf of the research volunteer. You will receive a copy of this consent form after it has been signed.

Permission Form for Clinical Case Report Sample
Generally, Clinical Case Reports regarding three or fewer experiences or observations identified during clinical care do not require IRB review. Submit the Not Human Research (NHR) form to obtain a written official IRB ruling as documentation for journal submission. Contact UKHC Corporate Compliance with HIPAA Authorization Questions.
Patient’s permission for sharing or publication of their medical case
Name of person described in report or shown in photograph: {Insert name}
Subject matter of photograph or report: {Insert subject matter}
Title of report or publication: {Insert title or report or publication}
Clinician or co-author: {Insert clinician or co-author name}
Clinician’s address: {Insert clinician's address}
Clinicians write case reports to share new, unique information experienced by a patient with other physicians and healthcare workers. Sharing the case may help other clinicians learn.
Factors to help you decide whether to allow your information to be used in this case report.
- Signing this consent form does not remove your rights to privacy.
- When we publish or present the case report, we will not include your name and other identifiers, but some characteristics about you may be shared.
- Specific information to be used may include: [specify what PHI will be accessed]
- The Information may be published in a journal that is read worldwide or online. Journals are aimed mainly at health care experts but may be seen by others, including journalists.
- We will take steps to keep your information confidential. However, we can’t guarantee that somebody somewhere, for example, a caregiver or relative, would not recognize that the report is about you.
- You will not directly benefit from the case report. However, the information may help the care received by others in the future.
- Allowing your information to be used will not cost you anything. Nor will you be paid or receive any reward.
- Allowing your information to be used is totally voluntary. Your decision will not affect your clinical care or treatment.
- If you change your mind at any time before publication, you can tell us in writing to the address above. Once the case report is published, it will not be possible to withdraw the consent.
- Take the time to make your decision and ask any questions that you may have.
I, {print full name}, give my permission for {insert name of clinician} to use and disclose my health information to write a case report about my (or my child/relative’s) clinical care and treatment.
Signature of Patient or Legally Authorized Representative: {Insert signature of patient or LAR} Date: {Insert date signature obtained}
Signature of requesting clinician/healthcare worker: {Insert signature of requesting clinician/healthcare worker} Date: {Insert date signature obtained}
This Authorization and Permission Expires: {insert date or event description}